Pain is a physical sensation. But it is also a psychological experience. It has a profound impact on our mind and emotions. Days filled with pain can lead to unnecessary depression, short tempers, and family conflict. Unmanaged pain can also slow healing and make it difficult to sleep.
Many patients and families worry about addiction to pain medicines. They also express concern about side effects. To be sure, it is best to start with nonprescription approaches to managing pain. If those don’t work, then gradually move to over-the-counter medicines. And then to prescriptions. In the case of serious illness, addiction is not much of an issue. Side effects are, but there are many ways to treat them.
Below are some thoughts to help you and your loved one as you navigate pain management decisions.
There are some situations where people are unable to use words to express that they are in pain. Those with advanced forms of dementia, for instance, can’t process words enough to answer the question, “Are you in pain?” People who are sleeping a lot or in a coma may be in pain but not able to say so verbally.
How can you know if your loved one is in pain?
While words may not be effective, sudden changes in behavior may signal that the person you care for is hurting somewhere.
Suspect pain if you notice changes in your loved one’s:
Breathing—becoming labored and noisy. As pain increases, breathing may become faster, including rapid, short breaths.
Body language—sudden restlessness, maybe pacing or sleeplessness. Fierce, even aggressive hitting, pulling or pushing away is frequently a sign of more severe pain. Curling up into a rigid ball is another common sign.
Facial expression—a new look of sadness or fear, or a scrunched-up, grimacing face can indicate your loved one is experiencing pain.
Ability to be soothed—the more severe the pain or discomfort, the less likely your loved one will calm down with simple reassurance or touch.
Speech or crying out—this is the most obvious signal. It includes soft moans or groans. Repeated yelling or wailing indicates there is intense pain.
It is difficult to describe the intensity of pain to someone else. The simplest way is to give it a score from 0 to 10. Zero represents no pain. Ten refers to unbearable pain. Assigning a number helps put the pain into an easy-to-understand perspective.
Many caregivers are surprised to discover that the person they care for downplays pain in front of the doctor. Even when he or she is asked a direct question about it, your loved one may deny having much pain when you know they have been hurting a lot. This can be confusing. A variety of reasons could explain your relative’s response.
They don’t want to seem weak.
They don’t want to be a “difficult patient.”
They fear that more pain means the disease is getting worse.
They don’t know how to describe what they are feeling.
Describing pain with a number can circumvent the tendency to downplay the intensity. It will give the health care provider the information needed to make appropriate recommendations.
Some families keep a log or diary to help track the pain. They note the day and time, the pain number, and any triggers.
Where might you store a log or diary so you can accurately track your loved one’s pain?
Massage
The healing power of touch has been recognized for millennia. Massage stimulates blood flow. It encourages relaxation and increases the recipient’s feeling of well-being. Great benefits can be obtained by light stroking, kneading, and rubbing. Seriously ill individuals may need the massage to be gentle and restricted to areas that are not red or inflamed. You may want to use lotion or oil to reduce friction on the skin.
Heat or cold
If a particular area of your loved one’s body is painful, consider hot or cold compresses. Ask your doctor which is most likely to be beneficial. A hot bath can help. Heat can also be applied by using electric heating pads, hot water bottles, microwavable bean bags, or gel packs. Tips to consider:
Be sure that the heat source is wrapped in cloth. You need to protect the skin from leakage or burns.
Heat therapy is best if it is applied for 20 minutes at a time.
If the person you care for is undergoing radiation therapy, do not apply heat to that part of the body.
For some types of pain, 15 minutes of cold is a better source of comfort. Ice packs, gel packs, or towels soaked in ice water all make excellent cold compresses. So does a bag of frozen peas. It conforms to the shape of the body. (Plus, you can keep refreezing it. Just mark it so you don’t forget and use it as food later!) As with heat therapy, be sure the source of the cold is wrapped to protect the patient against leakage or skin irritation.
Relaxation techniques
Relaxation techniques allow your loved one to interrupt the cycle of pain-fear-tension-more pain.
Deep breathing is slow, deliberate inhalation and exhalation of air. The emphasis is on the release of tension with each exhale.
Progressive relaxation involves tensing and then releasing muscle groups along the body. Start with the feet. Then the calves. Then the thighs. Work up the body gradually. By contracting muscles and then relaxing them, your loved one experiences the contrast. This makes it easier to deliberately release tension when pain is present.
Mental techniques for pain relief
Like massage, mindfulness exercises are recognized as an effective method of releasing tension and easing pain. There are several types.
Some focus on expanding the mind’s awareness beyond the level of the individual.
Others concentrate the mind’s awareness on the internal functioning of the body, for instance breathing in and breathing out.
Some exercises suggest focusing directly on the pain. Surprising as it may seem, really concentrating on what hurts, and where, can help it hurt less.
For those who are not inclined to mindfulness exercises, guided imagery can be very helpful. Guided imagery usually engages the imagination to “travel” to another place. Ask your loved one about a favorite scene or location. It could be a beach. Or a forest. Or a crisp mountain scene. Whatever is a special place for him or her. With a calm, low voice, describe images and sensations.
Sun on the face.
The smell of the trees.
The sound of a nearby brook.
A slow, detailed narration of this type can help your loved one by focusing attention away from the pain and onto pleasant and relaxing images.
What place or scene would your loved one like to “visit”?
Distraction
In the context of childbirth, Dr. Fernand Lamaze discovered the power of distraction. The nerve pathway that sends messages of pain to the brain can be filled with other nerve messages. This effectively distracts or blocks the brain from fully receiving the pain impulses. The Lamaze Method uses unusual breathing patterns and intense concentration to distract a laboring woman from the pain of her contractions.
This distraction principle is a useful one. If your loved one has nothing else to focus on, he or she is more likely to be fully aware of his or her pain. Alternatively, if he or she becomes engaged in an interesting activity or story, awareness of pain diminishes. Depending on your relative’s energy level, useful distractions can include
singing
playing cards
listening to music
watching television
talking with friends
reading
having a story read out loud
What distraction techniques might you use?
Reframing or adjusting self-talk
The experience of pain is multifaceted. It involves the mind’s awareness of a sensation in the body. It is also linked to our emotional reactions. Pain frequently brings up anger and hopelessness. The focus of our “inner voice” can deeply affect the way we feel pain. Your loved one can improve his or her ability to cope by reframing or altering any limiting or destructive messages.
For instance,
“Nothing has worked. This pain is never going away”
can be reframed to
“I wish I were not in pain. I guess I need to keep experimenting. Eventually I will find the right combination of approaches.”
Reframing intentionally shifts the awareness from what isn’t working to focusing on what is. It challenges all-or-nothing thinking.
“This is useless, nothing has worked”
can be transformed to
“This isn’t working as well as I had hoped. But ‘X’ has helped a little, and that’s a start.”
Perceived defeats cause a person to be more aware of pain. Perceived victories are empowering and reduce the perception of pain. Concentrating on what truly is working will give your loved one encouragement to move forward.
Talk with a specialist
Physical pain often brings with it emotional, spiritual, and social pain. Our perception of pain and our confidence in our ability to cope with it have a big impact on how much we suffer.
People in chronic pain are not able to be themselves. They are constantly distracted. Often they are irritable. They are frequently discouraged. Relationships can become strained. The person’s self-esteem can plummet.
Consider a counselor. Some people find it helpful to work with a counselor trained in pain management techniques. These professionals can help with coping strategies to offset the physical pain of illness. They can also offer suggestions for handling the complicated feelings that often arise when a person in pain is dependent on others for help and support.
Prayer or spiritual support
In times of pain, many people turn to their spiritual beliefs. They find it a source of great solace. If the person you care for is religious, it may help to pray, read scripture, or talk with a leader in your faith community.
Acupuncture
The Chinese have a long history of using acupuncture as a method to block pain. Acupuncture is based on the concept of “meridians.” These pathways in the body circulate vital energy, called “chi.” In the Chinese approach, pain is caused by blockages in these meridians. To relieve pain, an acupuncturist inserts very thin, sterile needles into specific junctures on the pathways. He or she twirls the needles to release the blockages. Once released, the balanced flow of chi is restored.
Which of these nonpharmaceutical approaches sound like something that would work in your situation?
Nonpharmaceutical approaches are the first line of defense against pain. And they will continue to help even if your loved one needs to turn to the use of medicines.
The next step up for relieving pain is over-the-counter drugs. These include drugs such as
aspirin
ibuprofen
acetaminophen
If the pain is very strong, your provider will likely suggest a medicine with morphine in it. These medicines are called “opioids.” They are extremely effective at relieving pain. Opioids come in several forms:
pills
liquids
patches
suppositories
pumps that inject a small quantity under the skin
fluids that are delivered through an IV
Side effects
Although opioids are very effective, they often cause side effects. This is why your relative’s provider will prescribe the lowest possible dose. Pinpointing the best solution may take some trial and error. Below is a list of the most common side effects caused by opioids and things you can do to relieve them.
Drowsiness, confusion, or delirium. With all drugs, there is a trade-off between the benefit of the drug and the side effects that come with it. Feeling sleepy is a common side effect of opioids. Often the pain has made it difficult to sleep, so some of that sleepiness is about “catching up.” After a week, sleepiness should not be as big a problem.
In addition to sleepiness, some patients experience confusion or delirium. (Delirium involves restlessness, confused or garbled speech, and sometimes seeing things that aren’t there.) Watch to see how intense your loved one’s reactions are before using opioids when he or she needs to stay alert for safety reasons (for example, driving).
Here are some things you to consider to reduce drowsiness, confusion, or delirium:
Ask for a smaller dose or an extended-release version.
Are other medications contributing to the problem? Many drugs list drowsiness as a side effect. Some may cause confusion or delirium, especially in combination with opioids. Could any of these medications be modified?
Is the pain relief adequate? Pain itself is tiring. It may be that the current medicine is not taking care of the pain well enough. Perhaps a different medication is needed.
Is a mild stimulant appropriate? Ask the health providers if caffeinated beverages would be okay. Is there an over-the-counter preparation that might help?
Call your provider if the symptoms are bad or if they come on suddenly after being on the medication for a week or more.
Constipation. Constipation is quite common. Opioids slow muscle movement, including the muscles of the intestines. Stool sits in the bowel longer, so more water gets absorbed. The stool then gets hard and difficult to pass.
Here are ways your loved one can avoid or prevent constipation:
Drink plenty of fluids. 8-10, eight-ounce glasses of water or nonsugar, noncaffeinated beverages per day.
Ask for a stool softener or laxative. Find out what preparation the doctor recommends.
Eat high-fiber foods when possible. These include vegetables, uncooked fruits (with the skins), and whole grains.
Sprinkle bran on food. Adding 1-2 tablespoons per day (along with drinking lots of liquid) can help keep the bowels moving.
Exercise when possible. Walking is the easiest exercise. Any movements that encourage action in the abdomen will help.
Sit upright to go. People who use a bedpan have more trouble with constipation than those who can walk to the toilet and sit upright. Consider a bedside commode if walking is too difficult.
Call the doctor if more than 2 days pass without a bowel movement.
Nausea and vomiting. As a general rule, nausea and vomiting will go away after a few days, once the body has adjusted to the opioids.
Medicines to help with nausea. There are medications designed specifically to reduce nausea and vomiting.
Changes to the medication schedule. Perhaps you can take less, but more often. Or maybe an extended-release version would create fewer side effects.
Is there a pattern? Some people notice that the nausea is worse if they are up walking around the first hour or two after taking the medication. In that case, it’s best to lie down for an hour afterwards to keep the nausea at bay.
Is the pain adequately relieved? Sometimes pain causes nausea. It may be that you need to try a different medication.
Are there other causes? Could other medications be contributing to the nausea? Is nausea a symptom of the condition itself?
Addiction to pain medicine is a serious public health problem. Many patients and their families are understandably concerned. The Centers for Disease Control has established tighter prescribing guidelines to curb this problem. They are very clear, however, that restrictions on pain medication should NOT apply to persons with cancer. Also that people receiving palliative care and persons who are near the end of life should not be denied pain medicines if they need them. People who have a serious illness simply are not affected in the same way as people who are healthy.
Below are corrections to some of the most common myths about the use of opioids for treating pain in the seriously ill.
Myth 1: Fear of addiction or dependency
Addiction is a physical dependence. It also includes a mental and emotional dependence that causes people to do things they know they shouldn’t. People with serious illnesses rarely become addicted to pain medicines. They do need the medicine for pain relief. They do not become consumed with receiving it.
Unfortunately, fear of addiction often results in family caregivers not giving enough medication. Or patients not asking for it when they need it. This can lead to your loved one experiencing unnecessarily high levels of pain. If you are worried about addiction, talk to your provider. He or she can let you know about the very, very low risks. Also ask about the signs of addiction and what to do. This might help you feel better about giving medication when it’s needed.
Do you have worries about addiction?
Myth 2: Fear of developing a tolerance
Some people are concerned that if their loved one takes pain medication too early, the body will adjust. Over time, they will need increasing dosages to get the same relief. This is called “developing a tolerance.”
It is true that dosages may have to be increased. Fortunately, in the context of a serious illness, gradual increases are okay. They will not cause an overdose.
That does not mean that there will not be any side effects from more medicine. Increased dosages may increase the number or severity of side effects. But if you are concerned that there will be no pain relief later, you do not need to hold off on giving the medicine now.
Do you have worries about your relative developing a tolerance?
Myth 3: Concern that more pain means the disease is getting worse
Your loved one might experience increased pain for a variety of reasons. In the case of a tumor, it may simply have shifted. Now it is pressing on a different set of nerves. Or, psychological circumstances may have changed. This may change the person’s perception of pain. For instance, relatives who were visiting have had to return home. Without the pleasant distraction of their company, your loved one is more aware of pain and discomfort.
No matter the reason for increased pain, if this change is not addressed, your relative is likely to experience unnecessary pain and distress. Talk with the provider if the pain is getting worse.
Stick to a regular schedule Some people try to stretch the time between dosages. This often causes breakthrough pain. It is much harder to bring pain back under control than it is to prevent it from flaring up in the first place. Going off the schedule can result in a need for more medicine overall.
Forgetting. If you are having trouble remembering to give a dose, use an alarm clock, cell phone, or the oven timer to remind you.
Fear of side effects. If the issue is side effects, check our tips listed above. Or talk to your health care provider. There may be alternative medicines that have fewer side effects.
Do not skip middle-of-the-night doses For pain medicines to work, the body needs a constant level of medication. Skipping doses in the middle of the night is likely to bring on avoidable pain. If getting up is too difficult, try shifting the schedule. See if you can set the late night and early morning doses to more realistic times.
How will you handle middle-of-the-night doses?
Get instructions about breakthrough pain
Sometimes a person will begin to feel pain before the next dose is due. Generally, it is better to give a smaller dose in the middle than wait until the next scheduled time. Ask your relative’s provider about the best way to handle breakthrough pain. It is easier to stop a buildup of pain than it is to correct it after the fact.
What is the plan for breakthrough pain?
If the patient vomits up the medicine
Some medications can be given again. Others require that you wait a specific period of time. If vomiting is a problem, ask for medication to reduce it. Or, talk with the provider about a different pain medicine. Or a different form. For instance, the medicine may also be available as a patch on the skin. No need to swallow!
What is the plan if your relative throws up the medicine?
Consider alternate forms of the medicine
Medication can often be delivered in several formats. If your loved one is having problems, check to see if these options are available:
Liquid drops under the tongue
A patch on the skin
A suppository
Crunching the pill up and eating it in applesauce
Use a pill tray
Many people with a serious illness take an overwhelming number of medicines. To help keep track, purchase a pill tray. Usually they have compartments for morning, noon, evening, and night. Choose a calm time to fill the box. A time with few distractions. Bring out all the medicines and fill the tray for the week. Once the tray is full, simply deliver the medicines one compartment at a time. You will find that using a pill tray also helps avoid skipped doses.
Call several days in advance for refills
It often takes a few days to get a doctor’s okay to refill a prescription. When your loved one gets down to five days’ worth of medicine, call the pharmacy. It’s better to be safe than sorry!
Use one pharmacy
Many patients have several doctors. It is difficult for these physicians to know what their colleagues have prescribed. Let the pharmacist help you avoid bad drug interactions. Have all your relative’s prescriptions filled at the same pharmacy. The druggist can alert you about combinations that are known to cause problems.
What pharmacy do you use?
Help monitor the pain
Keep a log of the types of pain your loved one is experiencing. Note when the pain occurs. What time of day? How long since the last medication? Any particular triggers or patterns you notice? Use a 0 to 10 rating system to describe the pain (0 = no pain, 10 = the worst pain imaginable). The more information you can give the provider, the more effectively he or she can help combat the pain.
Take periodic time away for yourself
It’s not selfish, it’s essential! Caring for a person in chronic pain can be very draining. If you do not take breaks, you are likely to burn out. Even just a simple walk around the block or lunch with a friend can do wonders to “refill your personal well.” Check with local agencies, friends, family, or your spiritual community for help. Patients on our service at Iowa City Hospice have access to professionals who can suggest local programs.
Give us a call at 1-800-897-3052, toll-free. You need to keep your strength up, if not for yourself, then for the sake of your loved one.
 There are some situations where people are unable to use words to express that they are in pain. Those with advanced forms of dementia, for instance, can’t process words enough to answer the question, “Are you in pain?” People who are sleeping a lot or in a coma may be in pain but not able to say so verbally.
There are some situations where people are unable to use words to express that they are in pain. Those with advanced forms of dementia, for instance, can’t process words enough to answer the question, “Are you in pain?” People who are sleeping a lot or in a coma may be in pain but not able to say so verbally.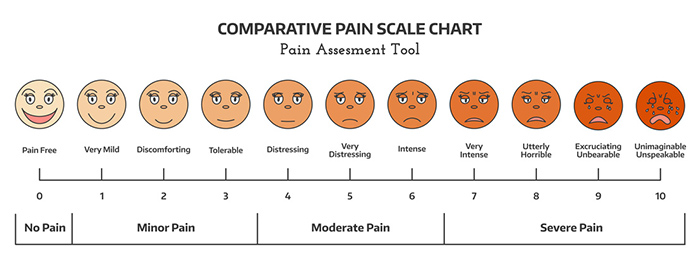



 If the pain is very strong, your provider will likely suggest a medicine with morphine in it. These medicines are called “opioids.” They are extremely effective at relieving pain. Opioids come in several forms:
If the pain is very strong, your provider will likely suggest a medicine with morphine in it. These medicines are called “opioids.” They are extremely effective at relieving pain. Opioids come in several forms: Drink plenty of fluids. 8-10, eight-ounce glasses of water or nonsugar, noncaffeinated beverages per day.
Drink plenty of fluids. 8-10, eight-ounce glasses of water or nonsugar, noncaffeinated beverages per day.